General Information on Outcomes Data:
The outcome data listed in this report includes data from all individuals who admitted to the DBT Institute of Michigan Residential DBT Program since program opening (4/1/2022 – 8/17/2025).
All clients included in these analyses had one assessment at the time of admission (completed within 4 days of admitting to the program) and at least one follow-up assessment score from a later date in treatment.
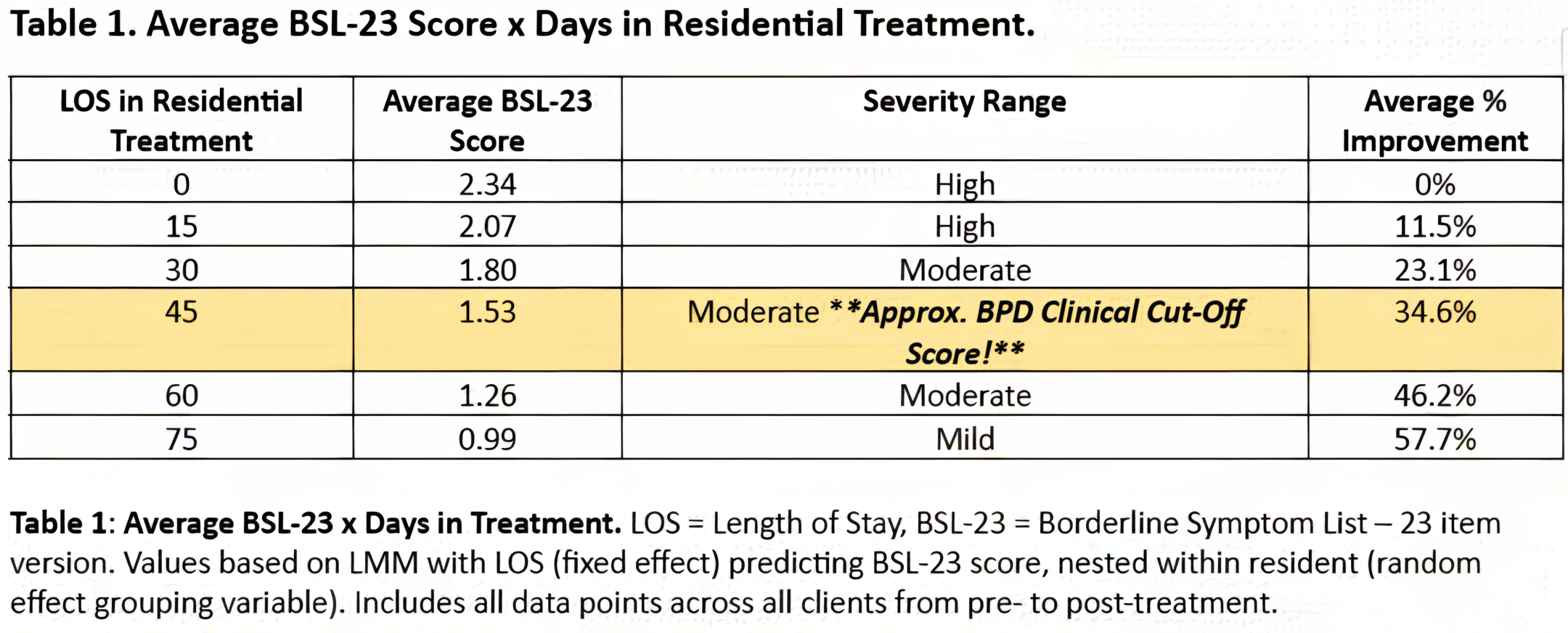
Linnear Mixed Models (LMM): Evaluates changes in self-report measures over time nested within each resident (Growth Curve Models). This maximizes statistical power as it takes all longitudinal data points into account vs. simpler pre-/post- designs and allowed us to cope with missing data points while still accounting for variability within and across residents. This approach is also more robust than pre-/post- designs against violations of statistical assumptions.
Models were fit using restricted maximum likelihood (REML) in JASP v.0.19.3.0 (JASP Team, 2024). Inferential tests for fixed effects were conducted using t-tests with Satterthwaite degrees of freedom (df). Satterthwaite df have been shown to be effective at controlling for Type I error rates when used with multilevel models (Luke, 2017).
Statistical analyses presented in the following report are results of Linear Mixed Models, which use all data points available – not specifically those identified by assessment phase (i.e., Admission, LOCF, Discharge, etc.).
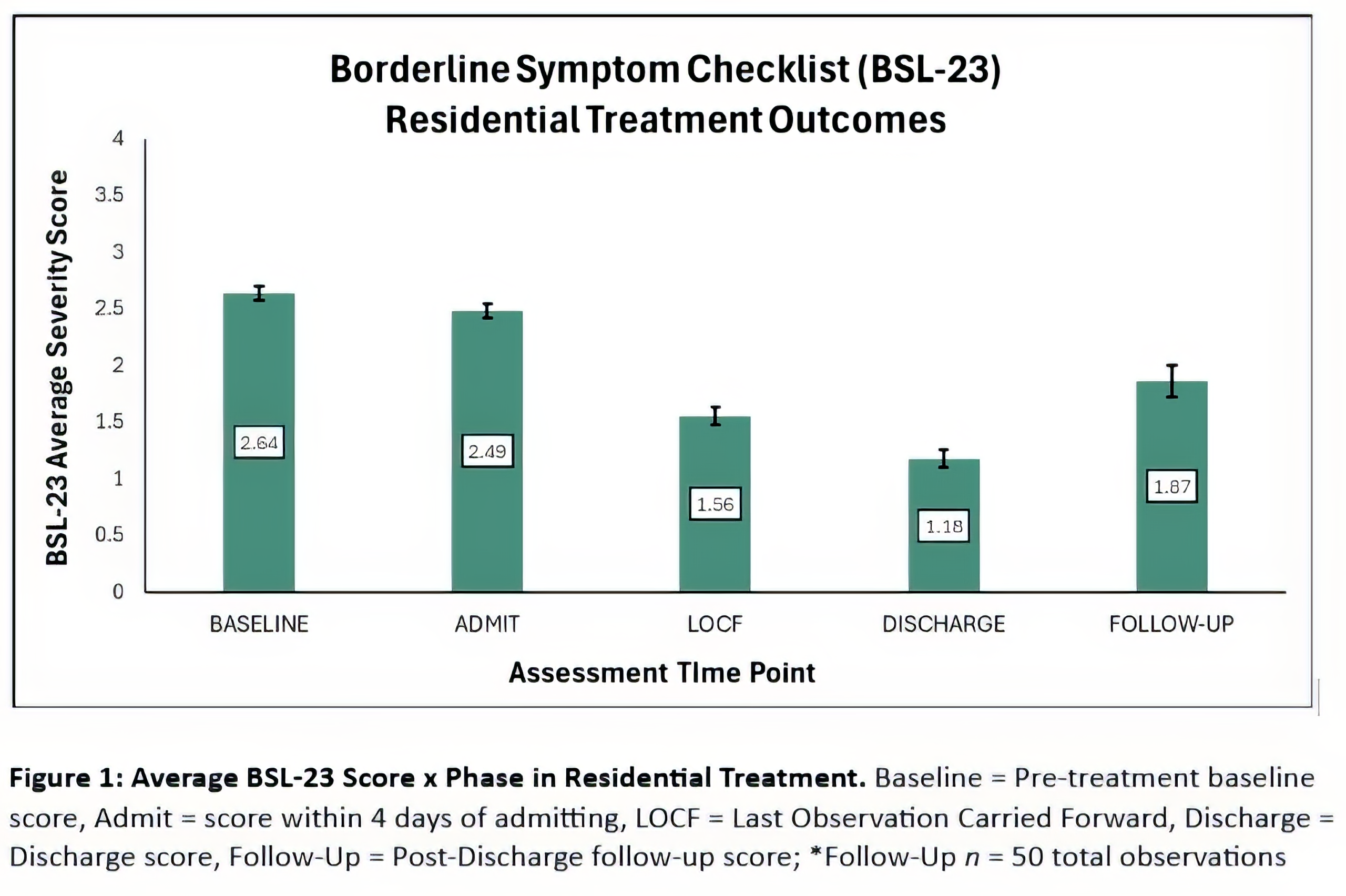
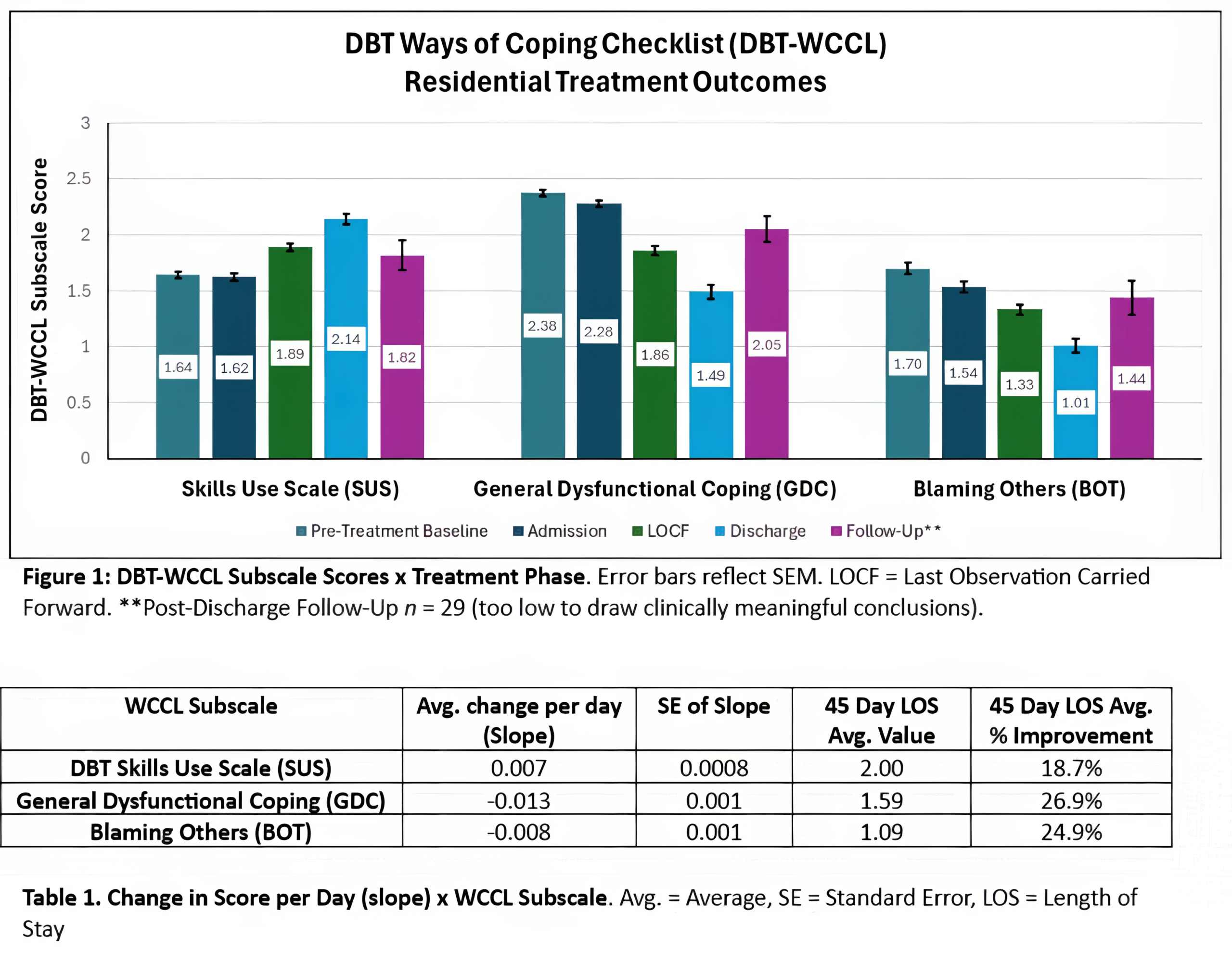
Graphs include specific assessment timepoints for data visualization purposes only. Statistical analyses were completed using all available data points.
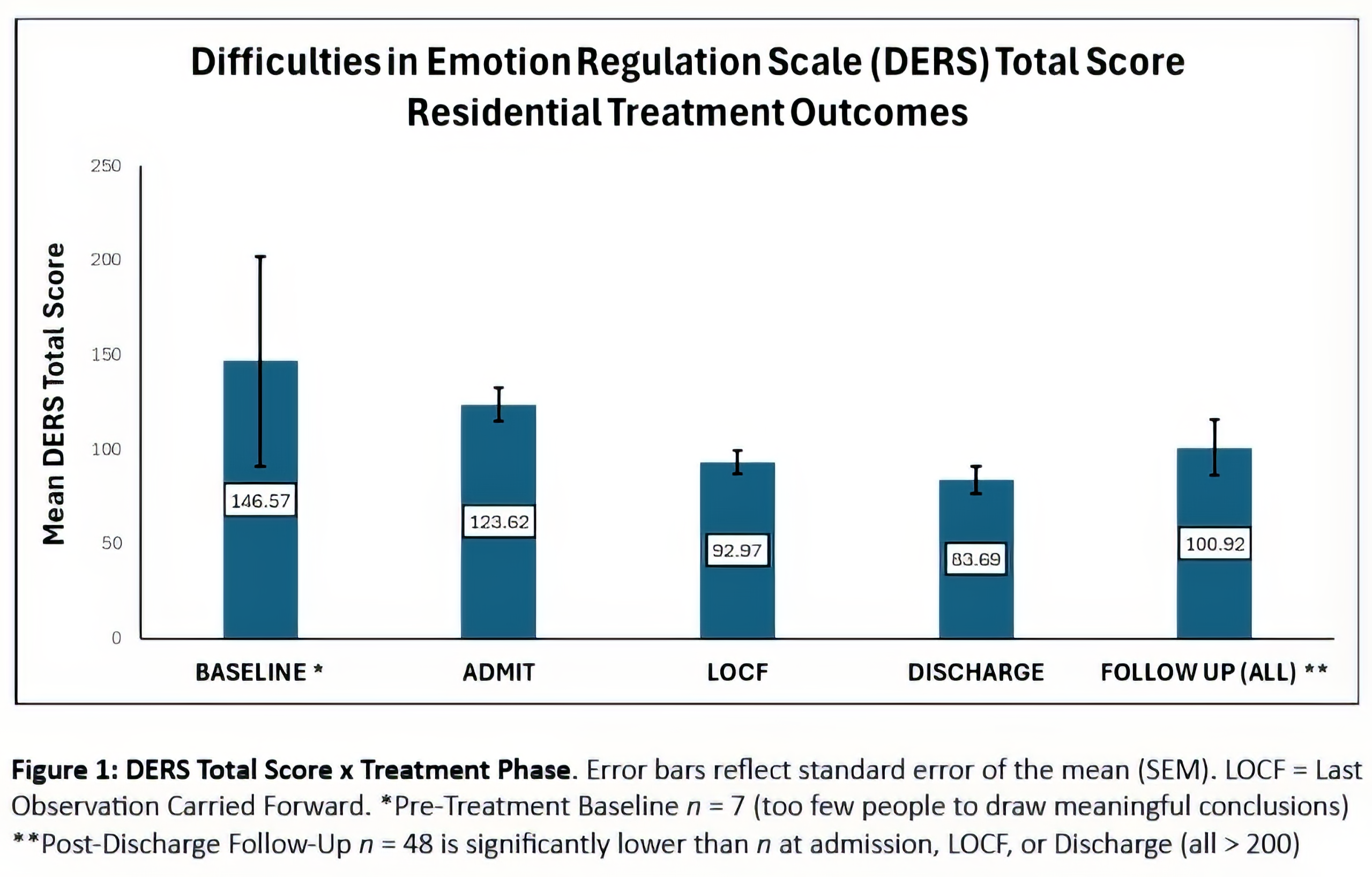
Last Observation Carried Forward (LOCF): Last observation carried forward is a common statistical approach to the analysis of longitudinal repeated measures data where some follow-up observations may be missing. In LOCF analysis, a missing follow-up visit value is replaced by that subject’s previously observed value – i.e., the last observation is carried forward.
Both LOCF and Discharge scores are included in graphs in this report as only including clients with documented discharge assessments would exclude a high percentage of all residents’ data. Moreover, it is unknown if the residents who completed discharge assessments are reflective of all clients’ end-of-treatment assessment scores on average vs. if there are confounding factors that make these groups different – i.e., clinical characteristics that contributing to abrupt or premature discharge causing missing discharge data.
Borderline Symptom List – 23 Item Version (BSL-23):
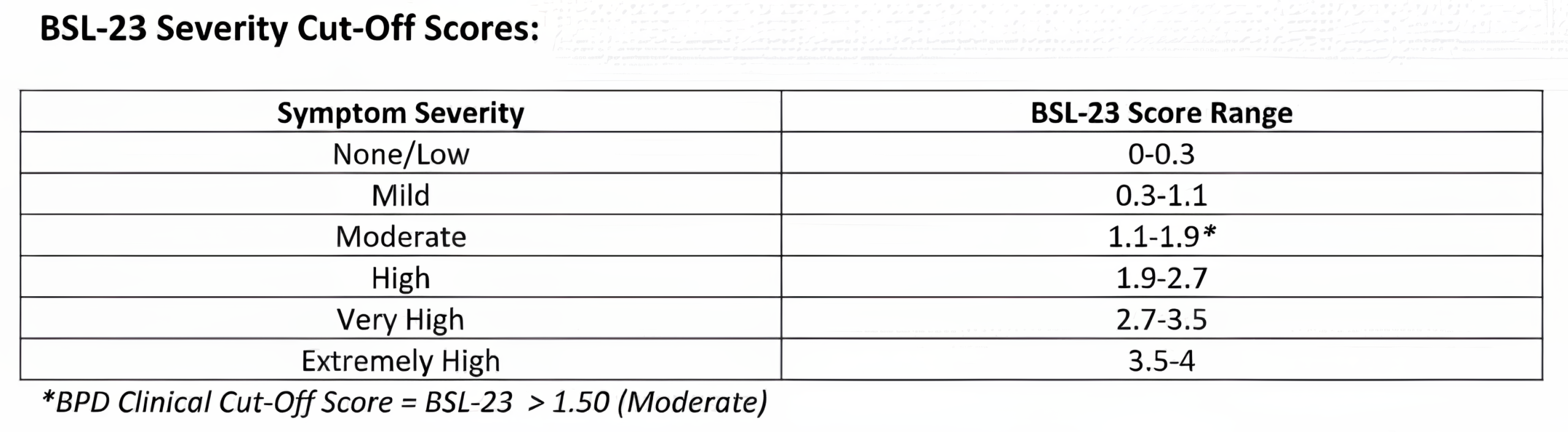
Description: The Borderline Symptom List-23 (BSL-23) is a 23-item self-report measure that is a reliable and valid self-report instrument for assessing symptoms of Borderline Personality Disorder (BPD). Items are rated from 0 (None at all) to 4 (Very strong).
Interpretation: Higher scores indicate greater BPD symptom severity. Clinical Cut-Off Score = 1.50+. This clinical cutoff score of 1.50 discriminates between clients likely to meet criteria for BPD vs. other psychopathology (Kleindienst et al., 2020).